





















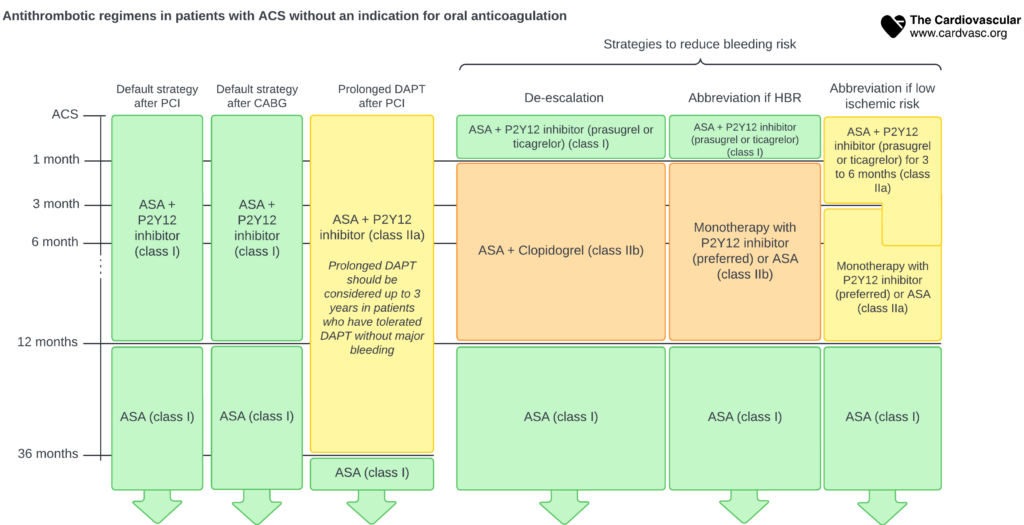
This diagram presents the recommended antithrombotic strategies for patients with Acute Coronary Syndrome (ACS) who do not have an indication for oral anticoagulation, categorizing them based on their treatment pathway and the duration of therapy.
• Default Strategy after PCI and CABG:
• 1 to 6 months:
• For both PCI (Percutaneous Coronary Intervention) and CABG (Coronary Artery Bypass Grafting) patients, dual antiplatelet therapy (DAPT) consisting of ASA (Aspirin) and a P2Y12 inhibitor is recommended (class I).
• 6 to 12 months:
• Continuation of ASA and a P2Y12 inhibitor is recommended (class I).
• Beyond 12 months:
• ASA monotherapy is recommended (class I).
• Prolonged DAPT after PCI:
• 6 to 36 months:
• Prolonged DAPT (ASA + P2Y12 inhibitor) is considered (class IIa) for up to 3 years in patients who have tolerated DAPT without major bleeding.
• Strategies to Reduce Bleeding Risk:
• De-escalation:
• DAPT with ASA and a P2Y12 inhibitor (prasugrel or ticagrelor) is recommended (class I).
• Alternative regimen: ASA and clopidogrel (class IIb).
• Abbreviation due to High Bleeding Risk (HBR):
• Monotherapy with a P2Y12 inhibitor (preferred) or ASA (class IIb).
• Abbreviation due to Low Ischemic Risk:
• DAPT with ASA and a P2Y12 inhibitor (prasugrel or ticagrelor) for 3 to 6 months (class IIa).
• Followed by monotherapy with a P2Y12 inhibitor (preferred) or ASA (class IIb).